When your child breaks out in a rash after starting antibiotics, panic is natural. You’ve done everything right - got the prescription, filled it, gave the medicine on time - and now there’s this angry red pattern spreading across their chest or back. Your first thought? Stop the antibiotic. But here’s the truth most parents don’t know: 9 out of 10 antibiotic rashes aren’t allergies. Stopping the drug unnecessarily can do more harm than good.
Most Antibiotic Rashes Are Not Allergies
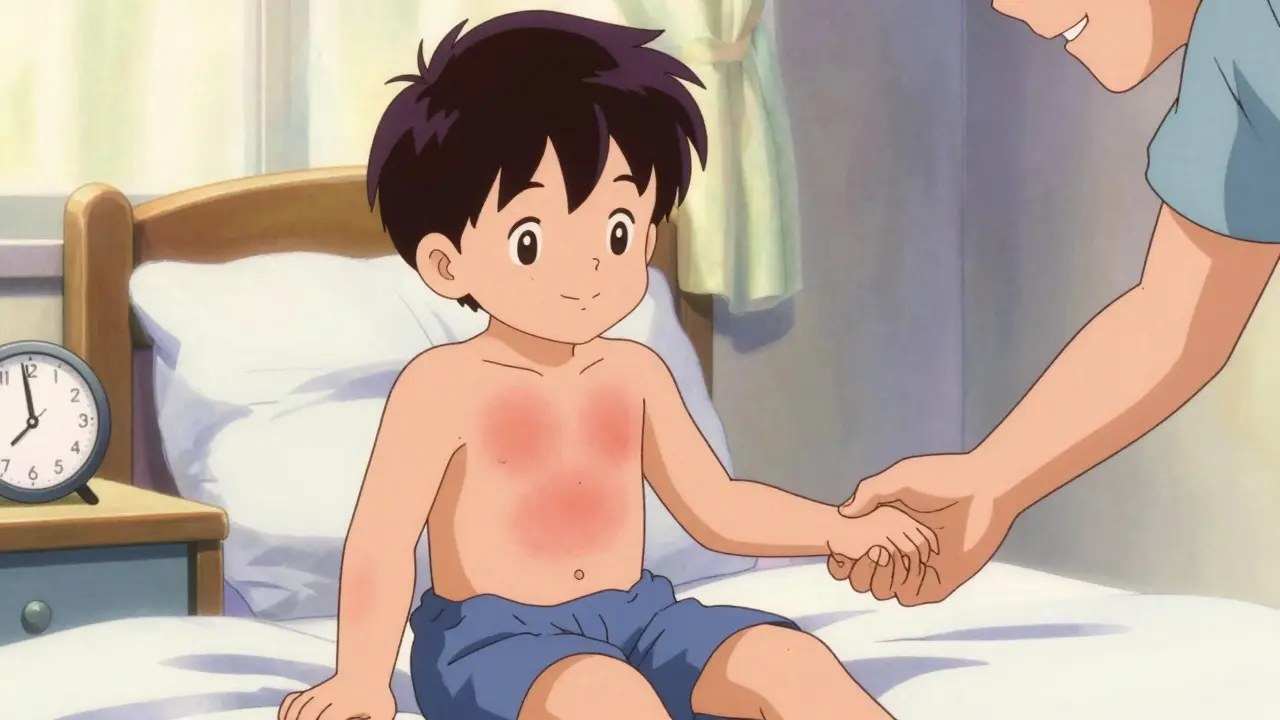
The most common antibiotic linked to rashes is amoxicillin. In kids, about 5% to 10% develop a rash while taking it. But here’s the twist: fewer than 1% of those kids are actually allergic. The rest? They’re having a non-allergic drug reaction. These rashes usually show up between days 5 and 10 of treatment. They look like flat, pink or red spots - sometimes slightly raised - scattered over the torso, arms, or legs. They don’t itch much, if at all. And they don’t move around. Unlike hives, which pop up in one spot, vanish, then reappear somewhere else, these stay put. Why does this happen? Often, it’s not the antibiotic at all. Many kids who get this rash are also fighting a virus - like Epstein-Barr (mononucleosis) or a common cold. The combination of virus and antibiotic triggers the rash. It’s harmless. It doesn’t mean their body is attacking the drug. It just means their immune system is reacting in a confusing way.How to Tell the Difference: Rash vs. Allergy
Not all rashes are created equal. Here’s how to tell if it’s just a harmless reaction or something dangerous:- Non-allergic rash: Appears after 5-10 days, flat or slightly raised, non-itchy, stays in one place, no fever, no swelling.
- Allergic rash (hives): Appears within 1 hour of taking the drug, raised, intensely itchy, changes location, often comes with swelling of lips or face, trouble breathing, nausea.
- Severe reaction (SJS/TEN): Rare, but life-threatening. Blisters, peeling skin, fever over 38.5°C, sores in mouth or eyes, rash spreading rapidly. This needs ER care now.
Why Stopping the Antibiotic Can Be Dangerous
When parents stop antibiotics because of a rash, they think they’re protecting their child. But the data tells a different story. According to the CDC, patients labeled as allergic to penicillin (often based on a rash they had as a kid) are 69% more likely to get a different, broader-spectrum antibiotic. Those alternatives? They’re stronger, more expensive, and harder on the gut. One study found that patients switched to other antibiotics because of a mislabeled allergy had a 63% higher chance of getting antibiotic-associated diarrhea. And a 30% higher risk of Clostridioides difficile - a nasty infection that causes severe, long-lasting diarrhea and can be fatal. In kids, stopping amoxicillin for a non-allergic rash leads to treatment failure 37% more often. That means the infection doesn’t clear. It comes back worse. Then you’re stuck with clindamycin or azithromycin - drugs that cause more side effects and contribute to antibiotic resistance.
What to Do If Your Child Gets a Rash
Don’t guess. Don’t Google. Don’t stop the medicine without talking to your doctor. Here’s what to do:- Take a photo. Document the rash. Note the date and time it appeared.
- Check for symptoms. Is your child feverish? Are their lips swollen? Are they having trouble breathing? Are they in pain? If yes - call the doctor right now.
- Don’t stop the antibiotic unless told to. If the rash is flat, non-itchy, and appeared after day 5, keep giving the medicine.
- Call your pediatrician. Describe the rash: "It’s flat, red spots on the chest, no itching, started on day 7." They’ll likely say: "Keep going. It’s common. We’ll monitor."
- For comfort: If there’s mild itching, use cetirizine (Zyrtec) at the right dose for their weight. Apply 1% hydrocortisone cream to itchy spots. Avoid scratching.
When to Call the Doctor Immediately
You don’t need to wait for a full-blown emergency. Call your doctor right away if:- The rash spreads quickly or turns into blisters.
- Your child has a fever over 38.5°C (101.3°F).
- Sores form in the mouth, eyes, or genitals.
- They’re coughing, wheezing, or have trouble swallowing.
- The rash is accompanied by swollen lymph nodes or joint pain.
What Happens After the Rash
If your child had a non-allergic rash, it will fade on its own in 5-7 days. The antibiotic will finish its job. The infection clears. The skin heals. No long-term damage. But here’s the next step most people miss: get the allergy label removed. If your child was told they’re "allergic to penicillin" because of a rash, that label sticks. It follows them into adulthood. It affects every future prescription. A 2023 study found that 92% of people who were labeled allergic based on a childhood rash could safely take penicillin again - if tested. Ask your doctor about a penicillin allergy test. It’s simple. A skin prick test, followed by an oral challenge if needed. Takes less than an hour. Many clinics now offer rapid 15-minute tests. It’s safe, accurate, and prevents years of unnecessary risk.Why This Matters Beyond Your Child
This isn’t just about your kid. Mislabeling antibiotic allergies costs the U.S. healthcare system over $1.2 billion every year. It drives up antibiotic resistance. It leads to more hospitalizations. It puts more people at risk for deadly infections. Hospitals that started testing patients for false penicillin allergies cut their use of last-resort antibiotics by 28%. They reduced C. difficile infections by 19%. That’s not just money saved. That’s lives saved.Bottom Line: Keep Going - Unless It’s Truly an Allergy
Most antibiotic rashes are harmless. They’re not a sign your child’s body is rejecting the drug. They’re a sign your child’s immune system is busy fighting a virus. Stopping the antibiotic because of it? That’s the real risk. If the rash is flat, non-itchy, and appears after day 5 - keep giving the medicine. Call your doctor to confirm. Take a photo. Monitor for fever or swelling. Don’t panic. If it’s raised, itchy, comes with breathing trouble, or shows up within an hour - stop immediately and seek help. And after it’s over? Ask about getting that allergy label removed. One simple test could protect your child for life.Is it safe to keep giving amoxicillin if my child has a rash?
Yes - if the rash is flat, red, non-itchy, and appears after day 5 of treatment. This is the most common type of antibiotic rash and is not an allergy. Stopping the antibiotic increases the risk of treatment failure and forces the use of stronger, riskier drugs. Always confirm with your doctor, but in most cases, continuing is the safer choice.
How long does an antibiotic rash last?
A non-allergic rash usually lasts 5-7 days after the antibiotic is finished. It may fade even while the drug is still being taken. Hives (true allergic reaction) may come and go over hours, but a maculopapular rash from amoxicillin doesn’t change location and fades slowly. If the rash worsens after stopping the drug, it’s not likely related to the antibiotic.
Can adults get antibiotic rashes too?
Yes. While less common than in children, adults can develop non-allergic rashes from antibiotics like amoxicillin, especially if they have a viral infection at the same time. The same rules apply: flat, non-itchy, appearing after day 5? Likely harmless. Raised, itchy, with breathing trouble? Stop and get help.
Should I give antihistamines for an antibiotic rash?
Only if the rash is itchy. For non-allergic rashes, antihistamines don’t speed healing - they just reduce discomfort. Cetirizine (Zyrtec) is safe for kids and adults. For true hives (allergic reaction), antihistamines help, but may not be enough. If breathing is affected, epinephrine is needed - not antihistamines alone.
Will my child always be allergic to penicillin if they had a rash once?
No. Only 1 in 10 children who had a rash on amoxicillin are truly allergic. The rest can safely take penicillin again. A simple allergy test - skin prick or oral challenge - can confirm this. Most doctors recommend testing before adulthood to remove the label and avoid unnecessary risks.



tatiana verdesoto
March 1, 2026 AT 01:24My daughter got a rash on amoxicillin last year and I panicked too. Turns out it was totally harmless - no itching, just red dots all over her torso. We kept going with the script and she recovered fine. Seriously, parents, don’t freak out unless there’s swelling or breathing issues. This post saved me so much stress.
Also, took the photo like they said. Best decision ever. Pediatrician looked at it and said, ‘Yep, classic.’ No drama. Just science.
Tobias Mösl
March 1, 2026 AT 15:39Let me guess - this is Big Pharma’s way of keeping you hooked on antibiotics so they can sell you more drugs later. You think they care about your kid? Nah. They care about the $1.2 BILLION in revenue from mislabeled allergies.
And let’s not forget - every time you ‘keep giving’ amoxicillin, you’re feeding a system that overprescribes. Antibiotics are not candy. They’re blunt instruments. And now we’re supposed to trust some CDC chart like it’s gospel? Wake up.
I’ve seen kids get rashes turn into full-blown autoimmune reactions. You think it’s ‘harmless’? Try telling that to the parents whose kids ended up in ICU because someone ‘followed the guidelines.’
Ethan Zeeb
March 3, 2026 AT 13:07As someone who’s been on the receiving end of a misdiagnosed antibiotic reaction - I’m calling BS on the ‘9 out of 10 aren’t allergies’ stat.
My son had a flat rash. We kept the meds. Three days later, his tongue swelled. We rushed him. Turned out it WAS an allergy - delayed onset. The guidelines don’t account for individual biology. You can’t reduce human immune responses to a spreadsheet.
If you’re unsure - STOP. Call your doctor. Don’t gamble with your kid’s airway because some study says ‘probably fine.’
Darren Torpey
March 4, 2026 AT 22:32Bro, this is the kind of post that makes me believe in humanity again.
You took the time to explain the difference between a ‘meh’ rash and a ‘oh-shit-I-need-epinephrine’ rash like a real doctor who actually cares. No jargon. No panic. Just facts wrapped in a hug.
My niece had that exact same rash - flat, no itch, day 6. We kept going. She’s now 12 and still takes penicillin like it’s water. No label. No fear. Just freedom.
Also - GET THE TEST. Seriously. It’s like getting your car’s VIN checked. You don’t wanna carry a fake ‘accident history’ for life.
Lebogang kekana
March 5, 2026 AT 05:17Listen, I come from a place where antibiotics are a luxury - not a right. We don’t have pediatricians on every corner. We have grandmas with herbal teas and neighbors who’ve seen it all.
But this? This right here? This is the kind of info that saves lives in villages where no one knows the difference between a rash and a death sentence.
I’m printing this out. Sharing it. Posting it on the community board. Because someone’s child is going to live because of this. Not because of a pill - but because someone took the time to explain.
Jessica Chaloux
March 5, 2026 AT 07:39OMG I JUST REALIZED MY KID HAD THIS RASH LAST YEAR 😭😭😭 I STOPPED THE ANTIBIOTIC AND NOW I FEEL SO GUILTY 😭😭😭 I DIDN’T KNOW 😭😭😭 WHY DIDN’T ANYONE TELL ME 😭😭😭
Mariah Carle
March 6, 2026 AT 09:29There’s a metaphysical layer here, you know? The rash isn’t just a biological event - it’s a mirror. It reflects our fear of losing control. We see red on skin and immediately assume the universe is rejecting us.
But what if the body isn’t fighting the drug… but trying to communicate? The rash is a whisper: ‘Something’s out of balance.’ Not an enemy. Not an allergy. Just… a signal.
Maybe the real cure isn’t the antibiotic - it’s the pause. The breath. The choice to not react out of terror.
Just saying. 🌿
Justin Rodriguez
March 6, 2026 AT 13:26Just wanted to add one thing: if you’re worried about the rash but not sure - take a picture every 12 hours. Compare. If it’s spreading *inward* or getting darker, that’s a red flag. If it’s fading or staying put? Good sign.
Also - don’t use hydrocortisone unless it’s itchy. It doesn’t fix the rash. It just masks it. And if you’re masking a real allergy, you might miss the warning signs.
And yes - get tested. I got mine at 32. Turned out I was never allergic. Saved me from 15 years of avoiding penicillin and getting C. diff twice. Worth the 45 minutes.